What is tennis elbow?
This is an excerpt from Sports Massage for Injury Care by Robert E McAtee.
Tennis elbow (lateral epicondylitis) is the most common overuse injury of the elbow, resulting from repetitive strain to the common extensor tendons of the wrist. Although this condition is named for a sport in which it's common, it can also occur in other activities that involve repetitive stress on the wrist extensors.
Signs and Symptoms
Lateral epicondylitis (or epicondylosis if no inflammation is present) is characterized by a deep ache at the lateral epicondyle that is made worse by activity. Other symptoms may include pain at the lateral elbow, mild to moderate swelling, and limitation of wrist extension or flexion. The athlete may also experience sudden twinges of extreme pain. In well-advanced cases, sharp pain is often reported when gripping a racket or even shaking hands.
Typical History
Tennis elbow, like most overuse conditions, develops gradually over several months. It may flare up suddenly as a result of increased intensity of activity, such as competing in a tennis tournament. If the injury is not the result of a racket sport, look for repetitive motion in the client's daily activities.
Relevant Anatomy
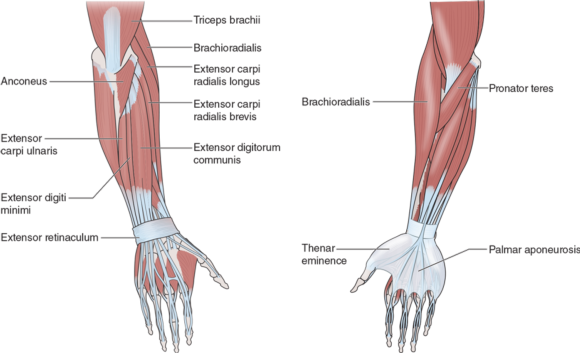
In most cases, the primary injury is tendinopathy of the extensor carpi radialis brevis (ECRB) tendon, just distal to its attachment on the lateral epicondyle. The rest of the wrist and finger extensors may be affected by the presence of tennis elbow, either by becoming hypertonic or by becoming inhibited because of pain. See figure 7.12 for illustrations indicating the wrist and finger extensors.
Extensor Carpi Radialis Brevis
The extensor carpi radialis brevis (ECRB) originates from the common extensor tendon at the lateral epicondyle of the humerus and inserts into the dorsoradial aspect of the base of the third metacarpal bone. Actions include extension of the wrist (with the ECR longus and ulnaris) and assisting radial deviation (abduction).
Extensor Carpi Radialis Longus
The extensor carpi radialis longus (ECRL)originates on the distal third of the lateral supracondylar ridge of the humerus, lying between the origin of the brachioradialis and the lateral epicondyle and inserts into the dorsoradial aspect of the base of the second metacarpal bone. Actions include extending the wrist (along with the ECR brevis and ulnaris) and assisting radial deviation (along with the flexor carpi radialis).
Supinator
The supinator originates from the posterior ulna, the lateral epicondyle, ligaments of the elbow and radioulnar joint, and the anterior capsule of the humeroulnar joint and inserts into the anterolateral aspect of the radius, just distal to the insertion of the biceps brachii. Actions include primary supinator of the hand and forearm; with the elbow flexed, the biceps brachii assists supination and assists elbow flexion when the hand is in neutral.
The radial nerve passes through the supinator muscle, and radial nerve entrapment may create symptoms similar to tennis elbow. Trigger points in the supinator may create referred pain that mimics tennis elbow and can be deactivated as part of the overall treatment for tennis elbow. Fun fact: Because supination is a stronger action than pronation, bolts and screws are designed to tighten by supination of the right forearm (righty-tighty, lefty-loosey).
Anconeus
The anconeus originates from the posterior aspect of the lateral epicondyle of the humerus and inserts into the lateral aspect of the olecranon process and the proximal posterior ulna. Actions include assisting triceps in extension of the elbow and assisting stabilization of the elbow joint during supination and pronation. The anconeus is thought to be secondarily involved in chronic cases of tennis elbow when additional stress placed on it results in compensation or inhibition of the extensor carpi radialis brevis.
Brachioradialis
The brachioradialis originates from the upper two-thirds of the supracondylar ridge of the humerus and inserts into the lateral radius, just proximal to the styloid process. Actions include flexion at the elbow, especially when the hand is in the neutral position; it may assist resisted pronation and supination. The brachioradialis may be secondarily involved with tennis elbow because of its proximity to the extensor carpi radialis longus.
Assessment
Observation
In severe cases, visible swelling over the lateral epicondyle may be present.
ROM Assessment
Active motion at the wrist consists of flexion, extension, abduction (radial deviation), and adduction (ulnar deviation). Depending on the severity of the injury, these motions may or may not cause pain. Passive motion is generally pain free except for wrist flexion, which may stretch painful tissues on the extensor side of the forearm, especially with the elbow extended.
Resisted extension of the wrist is painful. Resisted radial deviation may also be painful.
Manual Resistive Tests
The athlete, sitting or standing, places her wrist in neutral, forearm pronated. The examiner grasps the lateral elbow with one hand, and the other hand provides resistance as the athlete attempts to extend the wrist (see figure 7.13). This isometric contraction should begin slowly and build to a strong engagement of the target muscles. With the elbow flexed, the test will engage the ECR brevis more fully; with the elbow extended, the test will focus more on the ECR longus. Pain or weakness is a positive finding. Resisted extension of the middle finger (also known as Maudsley's test) is commonly positive for pain or weakness in tennis elbow (Fairbank and Corlett 2002) (see figure 7.14). If no pain occurs, the examination widens to include the other muscles that might cause lateral epicondyle pain, such as the supinator, brachioradialis, and anconeus.


SHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- How do I integrate nutrition education into PE?
- How does the support of friends and family influence physical activity?
- What makes the Physical Best approach unique?
- Strength training gimmicks . . . or not?
- How do vitamins and minerals support our bodies?
- Why do many people have difficulty losing weight?