Theory of Human Motivation
This is an excerpt from Essentials of Teaching Health Education With Web Resource, The by Sarah Benes & Holly Alperin.
The theory of human motivation (Maslow, 1943), better known as Maslow's hierarchy of needs, is considered a cornerstone of understanding human motivation. Even today it continues to be used as a foundation for other theories of motivation and behavior. The theory of human motivation asserts that we each have a set of basic needs that must be met, including biological and psychological, safety, belongingness and love, self-esteem, and self-actualization. Once our basic needs are met, such as having shelter or feeling loved, we are able to focus on our higher-order needs such as self-esteem and self-actualization.
Further research has expanded upon the original needs identified by Maslow to include three additional levels - cognitive, aesthetic, and transcendence. For the purposes of preK-12 health education, the original basic needs are more relevant for two main reasons. First, within the context of a health education classroom, educators must understand that whether or not a student's basic needs are being met will directly impact their ability to learn. Second, research on adolescent brain development notes the role that the prefrontal cortex plays in impulse control and decision making. It is unrealistic to expect adolescents to be developmentally able to move past these basic needs to a higher level of transcendence.
Maslow's hierarchy of needs is organized in a pyramid (see figure 3.1). The basic needs are at the base of the pyramid. As people meet their needs at each level, they are able to meet more complex needs, and they work their way closer to self-fulfillment and achieving their full potential. However, this is not a one-way process. People may find themselves revisiting levels based on life circumstances at a given time. This model provides a framework for understanding why people may be motivated toward certain behaviors at a given time; it does not provide specific steps that must be taken in order. The following sections look at each level in the hierarchy.
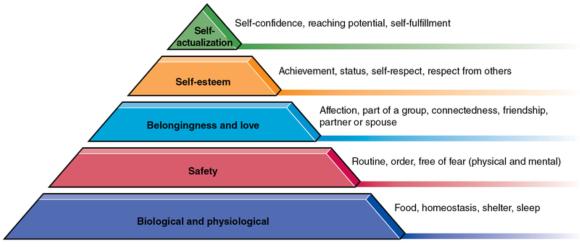
Maslow's hierarchy of needs.
Biological and Physiological Needs
The first level includes needs such as food, shelter, sleep, and homeostasis (the body's ability to maintain its natural state). These are the needs that are critical for survival. If they aren't being met, it is difficult to focus on anything else. For example, a student sitting in your classroom who has not eaten breakfast or is worried about where she's going to sleep tonight will have a hard time concentrating on learning.
Safety
In Maslow's hierarchy, safety expands beyond the physical to include emotional safety, order and predictability, routines, and stability. This includes being in familiar surroundings and not having to worry about a lot of unexpected change. In the classroom, a student may not be willing to participate in an activity or lesson, and as the educator you must consider whether or not resistance to participation is due to safety concerns (physical, emotional, or social) about participating. Will the student be teased for his response, is he afraid to try something new or unexpected, could he be physically hurt by the activity, or does the activity challenge his beliefs? Is there something going on at home that is preventing him from feeling safe and secure? If so, the student's reluctance may be rooted in a deeper issue and will likely only change if his safety concerns are addressed.
Belongingness and Love
Once a person is physically content and feels safe, the need to belong and be loved by others becomes important. The need for belongingness and love recognizes that each person needs more than just food and shelter. We need to belong to something greater than ourselves, to be part of a partnership or group that values us as an individual yet provides us with a sense of purpose greater than ourselves. This need may be met through nurturing friendships, having a trusted person to talk to, being in a romantic relationship, or feeling connected to a cause, such as a club or team. Belongingness and love are not necessarily taught to students. However, in health education we can teach students empathy, how to be a good friend, the difference between helpful and hurtful relationships, and assertive communication skills. We can also make the classroom a positive, supportive environment in which students feel a sense of safety and belonging. All of these feed into our need to belong and feel loved.
Self-Esteem
This level is best described as people having "a need or desire for a stable, firmly based, (usually) high evaluation of themselves, for self-respect, or self-esteem, and for the esteem of others" (Maslow, 1943, p. 381). We need to develop a respect of self that is fostered by an understanding of our own self-worth and abilities. If a student does not believe that she is worthy of being treated well, she is less likely to treat her body or mind well. Self-esteem also considers the need to be respected by others. It is connected to the self-efficacy (one's belief that one has the ability to reach a goal) aspect of SCT discussed in chapter 2. People with higher levels of self-esteem will likely also have higher levels of self-efficacy, which influences their ability to change or engage in certain behaviors. Teaching students the importance of respecting themselves and others is the foundation for developing skills to maintain or improve health. For example, we cannot expect students to set a goal for the future if they do not believe that they are able to control the outcome.
Self-Actualization
After all of the other needs are met, the need for self-actualization can be addressed. This need is based on the personal desire to do something substantial that helps us to reach our fullest potential. Specifically, self-actualization is about finding a sense of purpose in our work or actions. For students, this may be developing a plan and advocating for a cause that is important to them or choosing a behavior they wish to change and then establishing a plan to improve in that area. You must listen to what students are saying during discussions, watch how they are behaving in class, and look deeper at the meaning behind it all. Your students bring with them a variety of issues, concerns, and needs that, if not addressed, will hinder their motivation to succeed and ultimately their performance both in and out of class.
Developmental Levels and Motivation
As students move from kindergarten through grade 12, many changes occur physically, mentally, socially, and cognitively. During this time of growth, needs and motivations change in large part due to the changes associated with each developmental stage. The changes that occur during childhood and adolescence are both natural and necessary for students to become productive adults. Although changes are to be expected, not all students develop at the same rate and the effect that development has on needs and motivation is not the same for all students. However, understanding the developmental level of your students will allow you to teach lessons in a way that is relevant to the situations and needs of the students in the room (see Example of Tailoring Lessons, Assignments, Assessments, and Expectations to Students sidebar). You must also keep in mind that age and developmental level are not always aligned; for example, students might be physically mature or emotionally mature for their age. Understanding key characteristics of developmental levels can be helpful, but it does not replace the need to get to know your students and adjust instruction as necessary.
In the health education classroom, it is important to know not only what is developmentally appropriate in the social, mental, emotional, and physical domains but also what is to be expected in terms of behavior. For instance, typical behavior varies from age to age. In high school it is likely acceptable for students to meet up with their friends without an adult present, whereas in elementary school students are likely to need permission and are taken to meet friends by an adult who stays in the vicinity. Knowing this will allow you to tailor lessons, assignments, assessments, and expectations to make them reasonable and appropriate - in other words, relevant and authentic - for students.
The National Health Education Standards are presented by developmental stages (preK-grade 2 and grades 3-5, 6-8, and 9-12). They provide a basis for teaching skills at an appropriate level for each developmental stage. The performance indicators include behavioral outcomes that are characteristic of the developmental stage. When examining the standards, it becomes clear that, as students get older, developmental changes such as moving from concrete to abstract thinking, moving from reliance on adults to independence and autonomy, and the strengthening of reasoning skills are reflected in the behavioral outcomes for the skills (e.g., emphasis moves from identifying in younger grades to analyzing and evaluating in older grades). However, the standards do not provide a background for understanding key characteristics and considerations for each stage. In this section we examine the characteristics of each developmental level, including how to teach students based on their developmental stage and examples of what activities to teach based on the performance indicator of the National Standards.
First we provide an overview of developmental characteristics within each of the following stages: early childhood, late elementary, middle school, and high school. For each level, there is a discussion of characteristics and teaching considerations as well as tables that provide examples of National Health Education Standards within each developmental stage. This section is organized by the verb or action language (e.g., identify, analyze, evaluate) in the performance indicators of the standards across a sampling of skills within each level. We also provide examples of developmentally appropriate activities that could be used to address the verb of the performance indicator (i.e., ideas that would require the students to perform the verb). Note that not all performance indicators are listed in these tables for each skill, and the activities are not intended to be a direct match with the performance indicators listed. The goal of this section is to demonstrate how the performance indicators relate to developmental characteristics and ideas for the classroom.
Example of Tailoring Lessons, Assignments, Assessments, and Expectations to Students
During a class discussion at the high school level, students may discuss how they can avoid peer pressure to smoke while out with their friends and to instead avoid those situations or make an alternative plan that includes refusal language. At the elementary level, a similar discussion on peer pressure related to tobacco use may include practicing simple refusal messages, identifying allies, and knowing when to consult a trusted adult for help. This could also play out in the classroom during discussions about group and community norms of appropriate behaviors and choices. At the high school level, students may be asked to brainstorm community norms that promote or allow risky behaviors (such as returning to play after a concussion) and then strategies to change those unhealthy norms. At the elementary level, the brainstorm may be about how to be a good friend and to encourage students to create a school culture of respect and empathy. Age differences will also be apparent when developing requirements for student assignments, scenarios for learning activities, and expectations about the type and depth of information students should share with the class about their lives.
Learn more about The Essentials of Teaching Health Education.
More Excerpts From Essentials of Teaching Health Education With Web Resource, The

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- How do I integrate nutrition education into PE?
- How does the support of friends and family influence physical activity?
- What makes the Physical Best approach unique?
- Strength training gimmicks . . . or not?
- How do vitamins and minerals support our bodies?
- Why do many people have difficulty losing weight?