Sternoclavicular joint injury
This is an excerpt from Acute and Emergency Care in Athletic Training With Web Study Guide by Michelle Cleary,Katie Walsh Flanagan.
The sternoclavicular (SC) joint is the only place on the body where the upper arm attaches via bony articulation to the axial skeleton. This joint is a loose connection between the medial clavicle and manubrium of the superior sternum. It has a joint capsule, disc, and several ligaments in addition to the SC ligament—the intraclavicular ligament (between the two medial aspects of the clavicle, superior to the sternum) and the costoclavicular ligament, which maintains the stability of the clavicle on the ribs below. The SC joint is inherently unstable, and only a portion of the clavicle actually articulates with the manubrium, relying on the SC ligament to provide more stability.
Injury to the SC joint is one of the true medical emergencies in orthopedics. Just posterior to the joint lie the trachea and carotid arteries, and not too lateral from there, the subclavian arteries are located (figure 10.12). A posterior subluxation or dislocation can be a life-threatening emergency with compression on any of these structures.
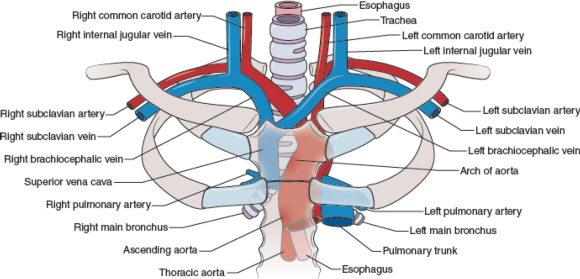
Figure 10.12 Internal structures behind the sternoclavicular (SC) joint.
Because of the SC's importance in connecting the arm to the body proper, the SC joint has many MOIs. One can fall on an outstretched hand or elbow, and the force can transmit along the bones of the arm, acromion of the scapula, and clavicle to the joint, injuring it. Another MOI is a fall on the lateral aspect of the shoulder (humerus or acromion of the scapula), or lying on one side with a pileup on the opposite lateral shoulder. In both of these situations, the force is transmitted along from the humerus/acromion to the clavicle and on to the biomechanically weakest aspect. The athlete could sprain the acromioclavicular joint or fracture the clavicle, or the force could continue medially and injure the SC joint at the sternum.
Incidence and Epidemiology
Injury to the sternoclavicular joint is rare, and posterior dislocations are more unusual. In a study of 251 SC dislocations, only 80 were posterior dislocations. Of the total number of dislocations (both anterior and posterior), the average age of the patient was 29 years old, and 67% of them were male.5 These data are consistent in other publications, in that younger males are more likely to sustain SC injuries than are other age groups or women.6
Risk Factors
Risk factors for injuring the SC joint include falling on an outstretched arm, elbow, or lateral shoulder. As noted, men under 30 years old tend to have higher incidences of SC injuries, so that population is at higher risk. Because high-velocity contact is a MOI, motor vehicle accidents are also a means of sustaining this injury.
Signs and Symptoms
When evaluating an injury to the upper extremity, it is important to be aware of the anatomical connection of the upper extremity and the SC joint. The athlete may initially feel more soreness at the point of impact (e.g., hand, elbow, shoulder) and not recognize the injury to the SC joint. Appreciating the MOI for a potential transmitted force to the medial clavicle and sternum is critical.
On inspection, a deformity may be present over the medial clavicle. It can range from mild swelling to gross deformity. A divot at the SC junction may indicate a posterior dislocation or subluxation, or a posterior fracture of the medial clavicular head (depending on the age of the athlete). Palpation results in a painful SC ligament or joint. Crepitus indicates a fracture, not dislocation or subluxation, but it is equally disconcerting.
Joint stress testing is not recommended, but sometimes the athlete presents with pain away from the SC joint, and that specific injury is not considered at the initial time of testing. The patient will present with an unwillingness to demonstrate full glenohumeral range of motion, because the stress on that joint affects the SC joint.
In a true posterior SC dislocation or subluxation, the patient may have dyspnea or hoarseness and relate difficulty swallowing, because the trachea is pushing posteriorly into the esophagus. If any of these complaints occur, consider it a medical emergency and transport via ambulance as soon as possible. On occasion, the patient will not identify the difficulty swallowing and hoarseness as related to the falling injury, and may not report these conditions. Anecdotal conversations with ATs indicate that athletes sometimes delay reporting issues of the voice or swallowing because they do not relate it to the SC sprain injury, only to have it be an emergency hours later when swelling increases and the airway begins to be compromised.
Field Assessment Techniques
Always assume a potential SC injury when presented with a mechanism consistent with the biomechanical weakness of the joint. Palpate all aspects of the clavicle, SC joint, and manubrium when evaluating falls resulting in landing on the outstretched hand, olecranon of the elbow, or acromion of scapula. If injury to the SC joint is suspected, assess airway and quality of voice. Ask the athlete to swallow, and query whether that action feels normal. Patients with swelling over the SC joint, who report that it is hard to swallow, or who have altered breath sounds, anxiety, or hoarseness should be removed from activity, have their shoulder pads removed (if wearing them), and be transported to the emergency department via ambulance. While waiting for transport, keep the athlete sitting up to facilitate breathing, and apply a sling to the affected arm. The sling will prevent unnecessary movement of the SC joint.
Reduction of the sternoclavicular joint is not recommended on the field. This procedure is performed under sedation or general anesthesia in an operating room. Open reduction and possible stabilization are necessary in situations of failed closed reduction or ongoing symptoms.7 Typically, surgical reduction of this injury is performed in conjunction with a cardiothoracic surgeon because of the potential for complications external to orthopedic surgery.
Diagnostic Accuracy
Standard radiographs of the SC joint are ineffective, because the X-rays are poor at viewing relevant anatomy of the joint.7 One technique that does provide better viewing is the serendipity view, which allows a 40° cephalic tilt.7 In this technique, an anterior dislocation presents as a superiorly displaced medial clavicle, and a posterior dislocation is represented as an inferiorly displaced medial clavicle.7 The preferred imaging is CT, which clearly defines the vascular and respiratory features that could be compromised.
Immediate Management Techniques
If the patient reports no difficulty with breathing or swallowing, but has swelling or tenderness over the SC joint, remove the patient from activity, place the affected arm in a sling, and reassess often. In this situation, ice may be held in place by the patient for 15- to 20-minute intervals if it relieves pain and swelling.
Indications
Dyspnea, hoarseness, or dysphagia following a collision or fall on an out stretched arm, elbow, or lateral shoulder are indications to transport the athlete via ambulance to the nearest ED.
Contraindications
Applying ice to the SC region after an acute injury may be contraindicated for a few reasons. The weight of the ice itself could put additional pressure on an unstable joint, further aggravating any dyspnea. Using a wrap to secure the ice to the area provides additional pressure to the area, which can actually worsen an unstable SC joint injury. The anatomical positioning of the trachea and major vessels from the heart immediately under the thin skin of the neck make ice an inappropriate treatment.
Criteria for Deciding to Transport for Further Medical Examination
Dyspnea, hoarseness, and difficulty swallowing following a collision or fall on an outstretched arm, elbow, or lateral shoulder are indications to transport the patient via ambulance to the nearest emergency department.
Transportation Techniques
Patients with a suspected posterior SC sprain should have supplemental oxygen available delivered via a nasal cannula. Transportation should occur in a recumbent position to facilitate easier respiration. A sling should be placed on the affected arm to relieve any traction of the SC joint from the weight of the upper extremity.
More Excerpts From Acute and Emergency Care in Athletic Training With Web Study GuideSHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- Machine learning: The cornerstone of data-driven decision making for sport organizations
- Examples of how systematic reviews and meta-analyses are used in sport
- Conjoint analysis: Determining why consumers choose one product over another
- Designing and conducting legal research in sport management
- Bilingual bites – Spanish terms for the cardiovascular system
- SOAP note section–specific terms for health care records