Risk factors for coronary artery disease
This is an excerpt from ACSM's Exercise Management for Persons with Chronic Diseases and Disabilities-4th by Geoffrey E Moore,J Larry Durstine,Patricia L Painter.
Hypertension and Dyslipidemia
Hypertension and dyslipidemia are separate independent risk factors for coronary artery disease (CAD), and in the United States, 33% of Americans have dyslipidemia and 29% have hypertension. These diseases frequently occur together, however, and the combination speeds the process of atherosclerosis. When both conditions are present, the likelihood of having clinically significant CAD is drastically increased because atherosclerosis develops in areas of arteries that experience high blood pressure when high levels of low-density lipoprotein (LDL) are present. Because of this interrelationship and the role of exercise in mitigating these two conditions, hypertension and dyslipidemia are discussed here as linked CAD risk factors.
Basic Pathophysiology
The basic pathophysiology of these conditions is closely interrelated but is discussed separately to highlight key issues.
Hypertension
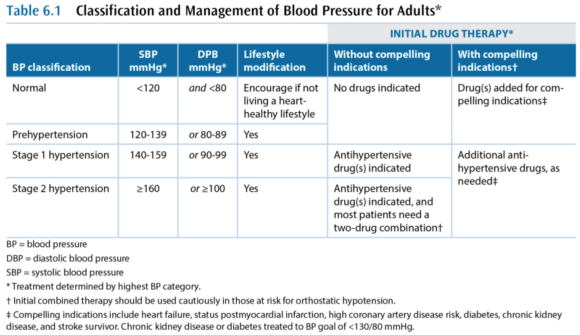
Hypertension (HTN) is a very common chronic condition, affecting about one in five people; it is defined as either
- systolic blood pressure (BP) over 139 mmHg or
- diastolic BP over 89 mmHg.
Table 6.1 has a more complete description of the classes of hypertension. High BP increases the risk for nonfatal and fatal cardiovascular disease, particularly CAD, kidney disease, and stroke. Even BP that is increased but not meeting the criteria for hypertension causes cardiovascular disease.
While hypertension is a common condition, the cause is not very well understood. In more than 95% of hypertension cases, the etiology is unknown and the condition is referred to as primary or essential or idiopathic hypertension. The remaining 5% of cases are secondary hypertension, so named because there is an identifiable underlying cause such as sleep apnea, drug-induced or drug-related causes (e.g., chronic corticosteroid therapy), chronic kidney disease, renovascular disease, aldosteronism, Cushing's syndrome, pheochromocytoma, coarctation of the aorta, and hyperthyroidism.
Dyslipidemia
Dyslipidemia - a high level of blood lipids - is a complex set of conditions, but the main concern is a high level of cholesterol. Cholesterol is critically important to every cell in the body, as a constituent of cell membranes that helps regulate their stability. Cholesterol is also an intermediary compound in steroid hormones, but the amount of cholesterol needed for hormones is many orders of magnitude lower than that needed for cell membranes. Cholesterol is synthesized and metabolized in the liver and then transported between the liver and the rest of the body. Cholesterol is not soluble in blood plasma and therefore has to be transported in the blood by lipoproteins. There are many different lipoproteins, each functioning to guide the cholesterol it carries to the proper metabolic pathway. This is the basic triad of lipoproteins:
- Very low-density lipoprotein (VLDL)
- Low-density lipoprotein (LDL)
- High-density lipoprotein (HDL)
The VLDL fraction carries about 80% triglycerides and 20% cholesterol, while the LDL and HDL mainly carry cholesterol. The total blood cholesterol is the sum of the cholesterol bound to VLDL, LDL, and HDL, and these cholesterol subcomponents are indicated with a -C suffix (e.g., LDL-C). Several subclassifications also exist, including two notable subclasses of LDL:
- Lipoprotein (a)
- Small dense LDL
Cholesterol metabolism is extremely complex, but the most important issue is that elevated total cholesterol and low-density lipoprotein cholesterol (LDL-C) are associated with an increased risk of CAD. Lipoprotein (a), or Lp(a), increases risk of CAD and of developing a thrombus, and small dense LDL also increases CAD risk. In contrast, high-density lipoprotein cholesterol (HDL-C) decreases CAD risk, through a cardioprotective effect that is partially related to this lipoprotein's role in the reverse cholesterol transport. In reverse transport, the cholesterol in HDL-C is transported to the liver where it is catabolized and excreted as bile.
Terms Often Used to Refer to Blood Lipids
- dyslipidemia - elevated triglycerides and cholesterol
- hypercholesterolemia - only cholesterol is elevated
- hypertriglyceridemia - only triglycerides are elevated
- exaggerated postprandial lipemia - prolonged elevation of triglycerides following consumption of dietary fat
- hyperlipoproteinemia or dyslipoproteinemia - high lipoprotein concentrations from genetic abnormalities or an underlying condition such as diabetes, renal disease, hypothyroidism, biliary obstruction, or dysproteinemia
Management and Medications
Medical management in persons who have the common chronic conditions often involves one or more medications for each condition, such that people with cardiometabolic conditions are often on five to eight prescription medicines. Again, this discussion treats these independently, but readers should expect to see multiple medications in persons in this group.
Learn more about ACSM's Exercise Management for Persons With Chronic Diseases and Disabilities, Fourth Edition.
More Excerpts From ACSM's Exercise Management for Persons with Chronic Diseases and Disabilities-4thSHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW