Physical activity recommendations for metabolic health
This is an excerpt from Foundations of Physical Activity and Public Health 3rd Edition With HKPropel Access by Harold W Kohl,Tinker D Murray,Deborah Salvo.
Figure 5.9 illustrates the relationship between the risks of having metabolic syndrome and the amount of self-reported physical activity and exercise from several studies evaluating a dose-response relationship (USDHHS, PAGAC 2008). As shown, metabolic syndrome risk drops dramatically with moderate amounts of self-reported physical activity and exercise.
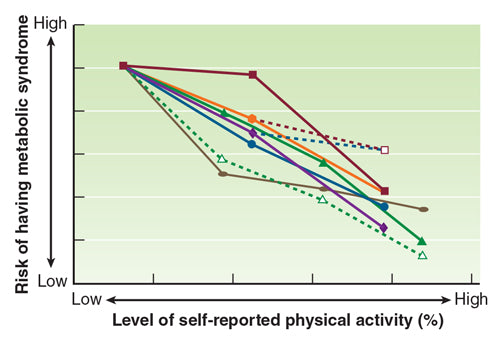
Reprinted from USDHHS, PAGAC (2008, p. G3-4).
Figure 5.10 illustrates the relationship between developing metabolic syndrome and levels of measured physical fitness from several studies evaluating a dose-response relationship (USDHHS, PAGAC 2008). Metabolic syndrome risk drops dramatically with moderate fitness levels for adults.

Reprinted from USDHHS, PAGAC (2008, p. G3-6).
In 2004, Dr. John Holloszy (a research exercise physiologist and public health professional) of the Washington University School of Medicine reviewed his career work of studying adaptations of skeletal muscle mitochondria for the ACSM (Holloszy 2004). In his review paper, Dr. Holloszy stated his belief that exercise deficiency is a serious public health problem with regard to the development of chronic diseases and the accelerated decline in the function of skeletal muscle, cardiovascular, and metabolic functional capacities with aging. He further asserted that the most important area of future research is to find effective ways to motivate “couch potatoes” to incorporate regular physical activity and exercise into their daily lives.
Evidence from the landmark Diabetes Prevention Program (2002) supports the lifestyle modification observations of Dr. Holloszy. Adults who were overweight and had prediabetes and who lost 7% of their body weight and were physically active 150 minutes per week reduced their risk for developing diabetes by 58%. The section that follows highlights recommendations from the PAGAC (USDHHS, PAGAC 2008) regarding the integration of physical activity and exercise science to promote metabolic health.
Scientific Evidence
The 2008 PAGAC reported strong and clear evidence that regular physical activity improves the metabolic health of at least moderately active people by 30 to 40% over that of sedentary people. The benefits of physical activity and exercise on metabolic health apply equally for men and women of all ages, and reasonable evidence supports the association for various racial and ethnic groups.
In 2008, the recommended dose to improve metabolic health was 120 to 150 minutes of moderate- or vigorous-intensity physical activity per week. However, evidence indicated that risk reductions were starting to be seen at levels below 120 minutes per week in people who engage in leisure time physical activity (LTPA). Evidence that resistance training was effective in treating diabetes was limited, although it did improve glucose control. It was noted at that time that more studies were needed to determine whether resistance training can prevent type 2 diabetes. Limited data existed regarding the effects of accumulated daily bouts of physical activity and exercise on metabolic risk, as well as whether physical activity helps control HbA1C or gestational diabetes.
The 2018 PAGAC confirmed the 2008 recommendations and expanded the review of the scientific evidence. The 2018 PAGAC reported the following with regard to physical activity and type 2 diabetes:
- Strong evidence demonstrates a significant relationship between a higher volume of physical activity and lower incidence of type 2 diabetes.
- Strong evidence demonstrates that an inverse curvilinear dose-response relationship exists between the volume of physical activity and incidence of type 2 diabetes, with a decreasing slope at higher levels of physical activity.
- Moderate evidence indicates no effect modification by weight status. An inverse relationship exists between a higher volume of physical activity and lower incidence of type 2 diabetes for people who have normal weight, overweight, or obesity.
- Limited evidence suggests that the relationship between a higher volume of physical activity and lower incidence of type 2 diabetes is not influenced by age, sex, race, or ethnicity.
- Insufficient evidence is available to determine whether the relationship between physical activity and the incidence of type 2 diabetes varies by socioeconomic status.
- Insufficient evidence is available to determine whether the relationship between physical activity and the incidence of type 2 diabetes varies by the frequency, intensity, duration, or type of physical activity, or how physical activity is measured.
The 2018 PAGAC also studied the scientific evidence regarding bouts of high-intensity interval training (HIIT; see chapter 2 for more) and the relationship between cardiovascular risk factors, weight loss, and metabolic profiles. The findings included the following:
- Insufficient evidence is available to determine whether a dose-response relationship exists between the quantity of HITT and several risk factors for cardiovascular disease and diabetes.
- Insufficient evidence is available to determine whether the effects of HITT on cardiometabolic risk factors are influenced by age, sex, race, ethnicity, or socioeconomic status.
- Moderate evidence indicates that weight status influences the effectiveness of HITT to reduce cardiometabolic disease risk. Adults with overweight or obesity are more responsive than adults with normal weight to HITT’s effects on improving insulin sensitivity, blood pressure, and body composition.
Guidelines
The guidelines for metabolic health are consistent with those for cardiorespiratory health for youth, adults, and older adults. However, people who may have metabolic syndrome or diabetes should take special precautions before undertaking physical activity or exercise programs.
Insulin concentration is an important determinant of the metabolic response to physical activity and exercise. The maintenance of glucose homeostasis is critical for all people, and a normal response to physical activity or exercise depends on exercise FITT (frequency, intensity, time, and type) variables, fitness levels, nutritional state, and environmental factors. For those with diabetes, other factors such as the use of insulin or other medications and the temporal relationship to eating are also important to consider during physical activity and exercise.
There are many ways to manipulate the timing and amount of insulin administration and food intake to avoid hypoglycemia or hyperglycemia. It is clear that a reduction in insulin dose in anticipation of exercise decreases the risk of hypoglycemia.
People with type 2 diabetes who are not treated with insulin and who do not have extensive vascular or neurological complications can generally exercise with no more concern than nondiabetic people of equal cardiorespiratory fitness. In addition to a preexercise evaluation, blood glucose monitoring should be performed during and after exercise to minimize the risk of developing hypoglycemia.
Added glucose ingestion prior to, during, or after exercise may be a more practical alternative to lowering insulin dose in the prevention of hypoglycemia. Table 5.2 provides some metabolic control guidelines for people who are active and insulin treated.

SHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- How do I integrate nutrition education into PE?
- How does the support of friends and family influence physical activity?
- What makes the Physical Best approach unique?
- Strength training gimmicks . . . or not?
- How do vitamins and minerals support our bodies?
- Why do many people have difficulty losing weight?