Help athletes stick to an injury prevention program
This is an excerpt from Psychology of Sport Injury by Britton W Brewer,Charles J Redmond.
Adherence to Sport Injury Prevention Programs
As discussed in chapter 3, recent years have brought a surge in attempts to prevent the occurrence of sport injuries. This surge has been accompanied by growing recognition of the vital importance of adherence both in preventing sport injuries and in documenting the effectiveness of preventive interventions (C.F. Finch & Donaldson, 2010; Van Tiggelen, Wickes, Stevens, Roosen, & Witvrouw, 2008). C.F. Finch (2006) asserted that in order to "prevent injuries, sports injury prevention measures need to be acceptable, adopted, and complied with by the athletes and sports bodies they are targeted at" (p. 5). Unfortunately, the extent of adoption and adherence by targeted groups and individuals has not routinely been considered in research studies (C.F. Finch, 2011). When adherence rates have been assessed, they have been found to vary considerably - ranging from not at all (Duymus & Gungor, 2009) to 100 percent (Heidt, Sweeterman, Carlonas, Traub, & Tekulve, 2000) - depending on the population under consideration and on how adherence was measured.
Although preventive efforts can involve administrators, legislators, and sport health care professionals, this part of the chapter focuses on adoption of preventive behaviors by athletes. Preventive behaviors that athletes may be encouraged to adopt include completing physical exercises (e.g., warm-up, stretching, strengthening, agility, jumping, balance), hydrating, wearing protective equipment, and doing stress management activities (e.g., Emery & Meeuwisse, 2010; Gissane, White, Kerr, & Jennings, 2001; Perna et al., 2003). The following sections address adherence to sport injury prevention programs in terms of measurement, theories, predictors, and enhancement of adherence.
Measurement
It is not possible to evaluate the effectiveness of sport injury prevention programs without knowing how well athletes adhere to the behavioral aspects of those programs. For example, if a program is found to be ineffective but the athletes did not adhere to it, then one cannot determine whether the program simply does not work or whether it would work if athletes adhered to it. Knowledge of adherence can be obtained only by operationally defining and measuring the construct. Consequently, both practitioners and researchers have a stake in measuring adherence.
Sport injury prevention activities can be implemented in both team and individual settings. The most common method of measuring adherence to sport injury prevention programs in team settings has been for coaches to keep a record of training sessions in which the prevention program was implemented and, in some cases, which athletes attended each session. These data can be used to calculate adherence indexes, such as the percentage of team training sessions in which the prevention program was implemented, the percentage of players on the team who completed a requisite number of training sessions that included the program, and a composite that accounts for both team and individual completion of prevention program sessions (e.g., Junge et al., 2011; Keats, Emery, & Finch, 2012; Soligard et al., 2008; Soligard, Nilstad, et al,. 2010; Sugimoto et al., 2012; van Beijsterveldt, Krist, van de Port, & Backx, 2011a, 2011c). Adherence to preventive activities completed on an individual basis - away from the team environment - has been assessed with self-report questionnaires (Chan & Hagger, 2012a; Emery, Rose, McAllister, & Meeuwisse, 2007).
Adherence reports from both coaches and athletes are subject to the usual potential limitations of self-report assessment - for example, forgetting, inaccuracy, andsocially desirable responses. However, in at least one investigation of the effectiveness of an injury-prevention training program, coach reports were verified and validated through monitoring by independent observers (van Beijsterveldt, Krist, van de Port, & Backx, 2011a). Independent observers have also been used to monitor and record athletes' use of protective equipment, such as headgear and mouth guards (Braham & Finch, 2004). On the whole, measurement of adherence to sport injury prevention programs is still in the early stages. More sophisticated measures are needed in order to capture aspects of adherence that are not typically examined (e.g., intensity of effort and use of proper technique during neuromuscular training) and to assess adherence more objectively (Chan & Hagger, 2012a).
Theoretical Perspectives
Theory helps us understand the processes by which athletes adopt preventive behaviors; it also guides the implementation of preventive interventions.
Until recently, the examination of adherence to sport injury prevention programs had been a largely atheoretical enterprise. Adherence had been assessed in epidemiological studies examining the prevalence of various preventive behaviors and in trials evaluating the effectiveness of prevention programs, but few researchers had made theory-guided attempts to understand why athletes adhere or do not adhere to the preventive activities. Indeed, a review (McGlashan & Finch, 2010) of 100 studies identified as investigating safety behaviors in association with sport injury prevention - the vast majority of which addressed the wearing of protective equipment - found that only 11 studies deployed theories or models from the behavioral and social sciences.
The onlytheoretical perspective used in more than two studies involved the theory of reasoned action (TRA; Ajzen & Fishbein, 1980; Fishbein & Ajzen, 1975), including its extension, the theory of planned behavior (TPB; Ajzen, 1991). When the TRA is adapted to behavior designed to prevent sport injury, it holds that the likelihood of engaging in preventive behavior is influenced directly by the intention to engage in such behavior. Intention, in turn, is affected by an athlete's attitudes toward the preventive behavior, as well as the opinions held by others in the athlete's social environment (i.e., subjective norms). In TPB, Ajzen (1991) added a third contributor to the athlete's intention to complete the preventive behavior - namely, the athlete's beliefs about personal control over the behavior. Therefore, from the perspective of TPB, adherence to sport injury prevention programs would be highest when
- athletes and their associates value the preventive behavior and its potential beneficial outcomes;
- athletes perceive themselves as having control over the preventive behavior; and
- as a direct consequence of the preceding two items, athletes intend to engage in the preventive behavior.
Noting the widespread support for TPB in the physical activity domain, Keats et al. (2012) advocated integrating it with self-determination theory (SDT; R.M. Ryan & Deci, 2000), a perspective thought to aid understanding of why athletes develop certain attitudes, beliefs, and intentions about behaviors designed to prevent sport injury. Specifically, athletes would be expected to value, perceive the support of others for, perceive control over, and intend to engage in preventive behavior when they experience satisfaction of basic psychological needs for autonomy, competence, and relatedness. Athletes experience autonomy when their decisions to complete preventive behavior are self-determined - that is, motivated by intrinsic factors (within the self) as opposed to extrinsic factors (outside the self). In addition, to the extent that the athletes perceive preventive behavior as being linked to sport success and favorable interpersonal relationships with important others (e.g., coaches, teammates), their needs for competence and relatedness are satisfied and TPB components conducive to adherence are elicited (Chan & Hagger, 2012b; Keats et al., 2012).
Figure 6.1 presents a graphic depiction of the model integrating TPB and SDT. Preliminary support has been found for SDT tenets in predicting athletes' motivation to engage in behaviors that reduce their risk of sport injury (Chan & Hagger, 2012a). With this in mind, an integrated approach such as that proposed by Keats et al. (2012) shows considerable promise as a means of understanding adherence to sport injury prevention programs and guiding the implementation of such programs.
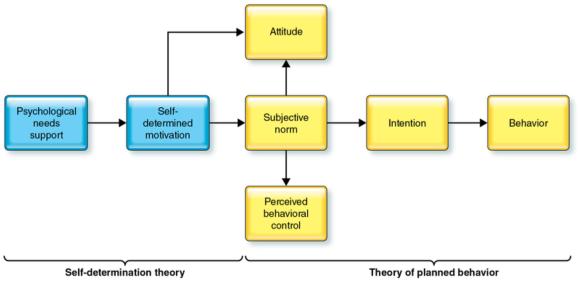
Model depicting integration of self-determination theory and the theory of planned behavior.
Sports Medicine, "Theoretical integration and the psychology of sport injury prevention, 42: 725-732, 2012, D.K. Chan and M.S. Hagger, Adis ©2012 Springer International Publishing AG. With permission of Springer.
Predictors
The general lack of theory-based research on factors associated with adherence to sport injury prevention programs has resulted in a hodgepodge of predictors of preventive behavior that lacks organizing themes. For the sake of discussion, the predictors can be divided into intrinsic factors and extrinsic factors, depending on whether they reside inside or outside of the individual. Intrinsic factors include injury history, personal characteristics, and cognitive variables. Athletes with a previous injury in a part of the body that can beprotected by a particular kind of equipment (e.g., lower extremity, eyes, mouth) have been found more likely than those without such an injury to wear protective gear during sport participation (Cornwell, Messer, & Speed, 2003; Eime, Finch, Sherman, & Garnham, 2002; Yang et al., 2005). With respect to personal characteristics, some evidence suggests that athletes who are older (Cornwell et al., 2003; Eime et al., 2002; Yang et al., 2005) or more experienced (Eime et al., 2002) use protective equipment to a greater extent than do their younger, less experienced counterparts - and that female athletes are more likely than male athletes to wear protective gear (Yang et al., 2005). For neuromuscular training, however, experience was inversely related to adherence for both coaches and athletes (McKay, Steffen, Romiti, Finch, & Emery, 2014).
The cognitive factors found to predict adherence to sport injury prevention programs include the intention to adhere, self-efficacy expectations, knowledge of injury risk, and a host of theoretically derived attitudes and beliefs. Athletes have been found to be more likely to wear protective gear when they are confident in their ability to wear the gear, intend to wear it (De Nooijer, De Wit, & Steenhuis, 2004), possess knowledge of injury risk (Eime et al., 2002), perceive fewer barriers to wearing gear, perceive themselves as susceptible to injury without gear, perceive injuries incurred without gear to be severe, and perceive more benefits to wearing gear (R.M. Williams-Avery & MacKinnon, 1996).
In the most extensive examination of adherence to sport injury prevention activities - which involved a sample of elite athletes in a variety of sports - Chan and Hagger (2012b) documented positive associations between a wide array of cognitive factors and a composite of behaviors considered to be protective against sport injury (e.g., warming-up, stretching, resting adequately, icing, taking supplements). Consistent with self-determination theory (R.M. Ryan & Deci, 2000), the study also found that greater self-reported adoption of protective behaviors was related to high levels of general factors such as satisfaction of basic psychological needs, self-determination for sport, and self-determination for injury prevention. Adherence was also positively correlated with several highly specific attitudes and beliefs. Some of the correlations were consistent with what would be expected, such as those involving beliefs about commitment to safety, worry about sport injury, and prioritization of injury prevention activities. Other correlations were the opposite of what would be anticipated, such as those involving attitude toward safety violations (i.e., viewing safety violations as sometimes necessary in pursuit of sport performance) and fatalism about injury prevention (i.e., viewing sport injury as unavoidable). Additional research is needed to clarify the nature of the relations between these specific attitudes and adherence to sport injury prevention activities.
Extrinsic factors associated with adherence to sport injury prevention programs include social influences and program and implementation features. In terms of social influences, athletes have demonstrated greater adherence to preventive behaviors when a large proportion of their teammates or friends are adhering (De Nooijer et al., 2004; Yang et al., 2005), when they perceive a high degree of support for autonomy (Chan & Hagger, 2012a), and when they report experiencing pressure from their parents to adhere (De Nooijer et al., 2004). Program and implementation features involve characteristics of prevention programs and the ways and contexts in which they are implemented with athletes. For example, athletes attending small high schools with low player-to-coach ratios have been found to wear protective equipment to a greater extent than do athletes at larger schools with higher ratios (Yang et al., 2005). Similarly, Australian squash players were more likely to wear protective eyewear when posters and stickers reminded them to do so and when the eyewear was readily available (Eime, Finch, Wolfe, Owen, & McCarty, 2005).
In the case of neuromuscular training programs designed to prevent musculoskeletal injuries, adherence is associated with the following program and implementation features: The program focuses on performance enhancement rather than injury prevention (Alentorn-Geli et al., 2009; Hewett, Ford, & Myer, 2006); it is not perceived by coaches as being too time consuming (Soligard, Nilstad, et al., 2010); and it is implemented by coaches (Hewett et al., 2006), especially those who have previously used prevention practices and perceive the athletes as highly motivated (Soligard, Nilstad,et al., 2010). Thus, athletes' level of adherence to preventive interventions is likely influenced not only by factors within the athletes themselves but also by other people and by characteristics of the interventions and their implementation.
Barriers to adoption of preventive measures, though not technically predictive of adherence to sport injury prevention programs, are directly relevant to adherence. To put it simply, when athletes perceive barriers to adherence, they may be less likely to adhere. In studies of the use of protective equipment (e.g., eyewear, headgear, mouth guards) during sport participation, athletes have identified a number of reasons for not wearing protective gear. Examples include cost (Chatterjee & Hilton, 2007; Pettersen, 2002), difficulty breathing (P.J. Chapman, 1985), difficulty communicating (C.F. Finch, McIntosh, & McCrory, 2001), dislike (Braham et al., 2004), restricted vision (Eime et al., 2002), transportationdifficulties (Chatterjee & Hilton, 2007; Pettersen, 2002), and discomfort (Braham, Finch, McIntosh, & McCrory, 2004; C.F. Finch et al., 2001; Pettersen, 2002; Schuller, Dankle, Martin, & Strauss, 1989; Upson, 1982).
Enhancement
Although adherence is becoming increasingly recognized as vital to the success of sport injury prevention programs, only limited attempts have been made to improve the potency of preventive interventions by enhancing adherence. One important step toward boosting adherence is that of incorporating behavioral theory into the design and implementation of sport injury prevention programs (McGlashan & Finch, 2010). Consistent with the recommendations of C.F. Finch (2006), more rigorous, systematic, experimental, theory-based exploration of factors associated with adherence can inform the development and evaluation of meta-interventions (i.e., interventions for interventions) - that is, procedures intended to facilitate adoption of and adherence to preventive interventions. For example, we can systematically manipulate key components of the model integrating TPB and SDT (described earlier in this chapter) and various predictors of adherence (identified in the preceding section) to determine features of prevention programs that optimize adherence to - and, ultimately, the preventive impact of - the interventions.
Learn more about Psychology of Sport Injury.
More Excerpts From Psychology of Sport InjurySHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW