Examining Posture
This is an excerpt from Examination of Musculoskeletal Injuries 4th Edition With Web Resource by Sandra J Shultz,Peggy A Houglum,David H Perrin.
Examination of Posture
Examine posture with the patient in a static position and in as few clothes as possible to allow an unobstructed view of all postural elements. (See the posture examination checklist later in this chapter.) Correct posture minimizes stress on muscles, bones, and joints while incorrect posture places abnormal stress on these structures. The more posture deviates from the correct position, the greater the stress placed on the structures that work to maintain it.
Incorrect posture usually develops with gradual changes in muscle, tendon, or fascial support. Children under the age of four generally have good posture and mechanics. As early as elementary school, children develop poor sitting and standing habits, and abnormal posture becomes apparent. By the time an individual becomes a teenager or young adult, abnormal postural habits are entrenched. Poor posture becomes more exaggerated as people age and develop progressively greater tightness and weakness in already shortened or lengthened soft tissue structures, resulting in changes in bone alignment and stress distribution.
Incorrect posture can also occur rapidly following an acute injury if the athlete alters position to reduce pain, functions with altered ability, or protects an injury. For example, a patient who experiences excessive swelling around the knee following an injury may not be able to stand with the knee fully extended, or a person suffering a cervical sprain may stand with the head thrust forward to relieve pain.
Sometimes an individual acquires an incorrect alignment because genetically determined joint or soft tissue characteristics cause the deformity over time, or the deformity present from birth becomes more apparent as the person ages.
You should include posture when examining any injury in the athletic training clinic. Posture can either result from injury or contribute to injury and should not be overlooked if you are to provide appropriate care. Examine posture by inspecting the anterior, lateral, and posterior views of the patient in the frontal and sagittal planes (figure 4.2).
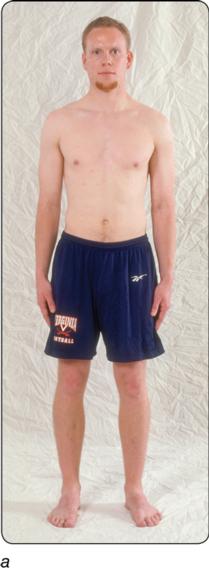


Correct standing alignment: (a) anterior, (b) lateral, and (c) posterior views.
Examination Procedure
A plumb line is often used as a reference of alignment for the body when examining posture. A plumb lineis a string suspended overhead with a small weight, or plumb bob, attached at the end near the floor. Position the patient behind the line so you can see the body bisected by the plumb line.
- Anterior view. The patient faces you with the plumb line dividing his body into right and left halves. Use the checklist for the anterior view to identify any deviations from normal.
- Lateral view. Observe the lateral view from both the left and right sides so you can see any imbalances between the two. Use the checklist for the lateral view to identify any deviations from normal.
- Posterior view. This view includes some of the same items observed in the anterior view but should not be eliminated since it also reveals other factors such as foot arch positions, knee fossa alignment, scoliosis, and scapula height. The plumb line bisects the body as indicated in the posterior view checklist. Again, use the checklist to identify any deviations from normal.
Postural Deviations
You should record postural deviations during the examination, ranking them as mild, moderate, or severe. Occasionally, a position may be considered normal, hyper-, or hypo-, while other postural deviations may be identified with names that define the abnormality but may not indicate severity. For example, genu recurvatum indicates hyperextension of the knee joint without relating the severity of the hyperextension. Placing a descriptor such as mild in front of these names can further qualify or quantify the deviation.
The examination process always includes comparison of left and right corresponding segments, because "normal" is often solely determined by comparison to the contralateral side. Normal for one person may not be normal for another person. For example, a gymnast will have much greater excursion in a straight leg raise than a baseball player, and a pitcher will have more glenohumeral lateral rotation than a first baseman. Each athlete must be compared only to herself and not to others.
Postural deviations cannot be recognized as abnormal unless normal posture is identified. You must know what is normal, or expected, in postural examination from all views. In part II, where the body regions and their associated injuries are discussed, postural deviations unique to those regions are presented. How to identify, treat, or modify the deviations, as well as the consequences of the deviations, are also discussed.


Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW
Latest Posts
- What performance obstacles do master athletes face?
- Cannabidiol (CBD) and mycoprotein as supplements
- Weight, body composition, and performance in athletes
- The gut-brain-bone axis and Biodynamic Skeletal Therapy
- Touch-testing in Biodynamic Skeletal Therapy treatment
- The six stages of Biodynamic Skeletal Therapy treatment