Causes of Sudden Cardiac Death in Athletes
This is an excerpt from Medical Conditions in the Athlete 3rd Edition With Web Study Guide by Katie Walsh Flanagan,Micki Cuppett.
Death by sudden cardiac arrest (SCA) is a rare event in the young athlete. In the United States, elite athletes are viewed as near invincible because of their incredible physical feats. Nevertheless, it is reported that the rate of collegiate athlete death due to SCA is higher than that of high school athletes, with a suspected 110 SCA deaths annually in the United States among young athletes (Casa et al. 2012). Any time a tragedy of this proportion occurs, the public reacts with disbelief, and medical knowledge is called into question. Studies that have tracked these deaths during sports used the National Federation of State High School Associations (NFHS), the National Collegiate Athletic Association (NCAA) governing organizations, and state and federally funded research groups for data collection, such as the National Center for Catastrophic Sport Injury Research (NCCSIR), based in Chapel Hill, North Carolina. Approximately 90% of the data collected involved male athletes, with an equal distribution between Caucasians and African-Americans (Borjesson and Pelliccia 2009). According to the NCCSIR, there were 10 indirect (due to exertion) fatalities in middle school through college football athletes in 2014, and six were attributed to a cardiac event (Kucera et al. 2015). An additional five football athletes died of suspected cardiac conditions due to nonexertional factors in the same year (Kucera et al. 2015). Sudden death cases in young women are rare, and the most common cause of sudden cardiac death was congenital cardiac disease.
The prevalence of sudden cardiac death in young athletes (those less than 35-year-old) is estimated to be between 1 and 3 in 100,000 (Borjesson and Pelliccia 2009). This is much higher than statistics reported in a more general population of active individuals (Harmon, Klossner, and Drezner 2011). These data indicate that active people are not immune to cardiovascular events that may result in death.
Causes
The most common cause of sudden cardiac death in the young athlete is hypertrophic cardiomyopathy, which accounts for up to 50% of the cases. Other significant causes of sudden cardiac death in a young athlete are coronary artery anomalies, increased cardiac mass, aortic rupture, myocarditis, and aortic stenosis(Borjesson and Pelliccia 2009).Rare causes include dilated cardiomyopathy, atherosclerotic coronary artery disease, mitral valve prolapse, isolated arrhythmias such as long QT syndrome and Wolff-Parkinson-White syndrome, and arrhythmogenic right ventricular dysplasia (ARVD) (Harmon, Klossner, and Drezner 2011). In the Veneto region of Italy, researchers have found ARVD to be the most common cause of sudden cardiac death in the athlete (Thiene et al. 1988). This research suggests that a specific population may have different genetic subtraits.
In the older athlete, coronary artery disease is by far the most common cause of sudden death. Rarely is sudden death in the older athlete caused by hypertrophic cardiomyopathy, mitral valve prolapse, or acquired valvular conditions (Maron et al. 2014; Nagashima et al. 2003; Semsarian, Sweeting, and Ackerman 2015; Marijon et al. 2015).
Traumatic sudden cardiac death has not captured as much attention because its epidemiology is more difficult to track. However, it is a growing problem that strikes without warning. Between 1996 and 2007, a reported 180 cases of blunt-force death in the United States were attributed to commotio cordis (Maron et al. 2006). Most cases involved children with a mean age of 13, with 95% of the deaths occurring in males (Maron et al. 2013).
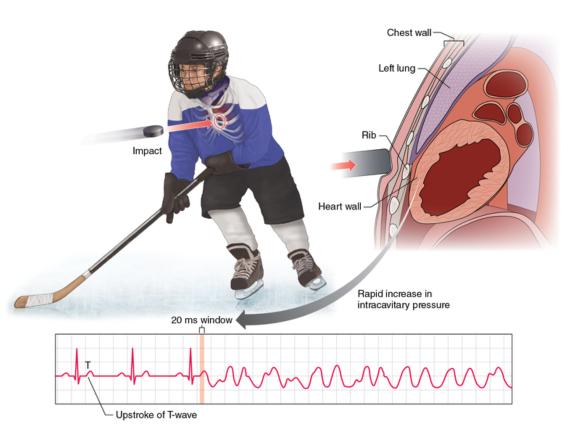
Commotio cordis refers to trauma to the chest wall that interrupts the electrical impulse in the heart. If the cardiac rhythm is not promptly normalized, the individual dies. Typically the ribs or sternum is not broken, although some contusions may be found. Research has found that a chest blow occurring during the vulnerable phase of repolarization, just prior to the T-wave peak in the cardiac cycle, can induce ventricular fibrillation (Maron and Estes 2005).
Although children and teenagers with thin chest walls are most vulnerable to commotio cordis (figure 8.6), deaths have been reported in adults. Sports such as baseball, ice hockey, lacrosse, and softball, which have hard projectiles that can strike the chest, have been associated with the greatest number of deaths. Commotio cordis also has occurred in sports such as soccer, football, rugby, and karate, in which the blow came from a soft projectile or a collision. It appears that the timing of the incident, rather than the degree of impact of the object, is the causative factor (Maron and Estes 2005). Commotio cordis is the only significant cause of traumatic sudden cardiac death in athletes.
The type of injury associated with commotio cordis is a blow to the chest wall that interrupts the usual cardiac rhythm.
Red Flags for Traumatic Sudden Cardiac Death
Sports with projectiles that can hit the chest at an inopportune time in the cardiac rhythm cycle have been known to cause commotio cordis in young athletes. These sports include the following: baseball, softball, hockey, lacrosse, soccer, football, karate.
Prevention
Because death can be the outcome, prevention has become the focus of attention for commotio cordis. Changes in practice have ranged from protective padding to softer balls that are used in Little League and softball. Because this may not completely resolve the problem, another solution is defibrillation in conjunction with cardiopulmonary resuscitation (CPR). Defibrillation interrupts the heart rhythm so the heart can "reboot" into a normal rhythm.
The American Heart Association estimates that communities with comprehensive CPR and automated external defibrillator (AED) training achieve 40% survival rates for cardiac arrest victims. If defibrillation is performed within 3 min, the likelihood of survival is high. For every minute of delay the chance of survival drops by as much as 10% (American Heart Association 2013).
The advent of the AED has provided greater public access to life-saving technology. These devices can be operated by trained laypeople and are increasingly affordable in all sectors. The AED is portable, rechargeable, simple to operate, and easy to maintain. The American Red Cross, American Heart Association, and National Safety Council offer AED certification courses in addition to CPR courses for the lay public. The NCAA Sports Medicine Guidelines require planned access to an AED and mandating CPR and first aid certifications for all who work with athlete practices, competition, and skill sessions. Athletic trainers are required to maintain certification in emergency cardiac care, including AED use. They need to have ready access to an AED in order to provide rapid cardiac assessment and care to those in fibrillation. Athletes who suffer a sudden collapse and have agonal or gasping breathing should be treated because they are suffering from a cardiac event (Casa et al. 2012; Solberg et al. 2015). An AED should be applied as soon as possible for heart rhythm analysis and possible defibrillation.
Clinical Tips
Potential Causes of Sudden Death
Sudden collapse in athletes could be caused by heatstroke, a cardiac event, sickle cell collapse, or injury. Understanding the presentation of each will facilitate rapid response and the appropriate disposition.
Emergency Planning
Every athletic site should have planned access to an AED, an emergency medical service (EMS), and an established emergency action plan (EAP), as well as medical personnel trained to respond to sudden collapse.
Learn more about Medical Conditions in the Athlete, Third Edition.
More Excerpts From Medical Conditions in the Athlete 3rd Edition With Web Study GuideSHOP

Get the latest insights with regular newsletters, plus periodic product information and special insider offers.
JOIN NOW